

Improving your communications with colleagues
A key to safe and rewarding practice

Information: the glue holding the structure together
Professionally as doctors we make decisions, record what we have done and let others know (not always in that order).
This post is concerned with the second and third of these, because much important information is “lost in communication” and never reaches its destination.
As in other spheres of human activity, numerous errors and misunderstandings in the practice of medicine follow failures in communication. We have all been guilty; I can think of occasions when I failed to communicate adequately with other doctors and healthcare professionals.
NHS England defines communication as ‘a two-way process…..in which participants not only exchange information but also create and share meaning’.
This implies that for the information to have meaning, the person sending the information should suggest an interpretation of it, and should receive an acknowledgement and comment from the recipient.
Widespread use of fast, concise and auditable communications between doctors, patients and other health professionals would make our everyday work much easier and safer. In this post I am going to focus on communication between doctors. However everything I say applies equally to doctors’ communications with other health professionals.
The default (often erroneous) assumption is that doctor to doctor communication is well-developed. I wish that were true.
Failure of communication:
My understanding of the term “failure of communication” is that it usually means an omission to hand on relevant information.
Sometimes failure of communication hides in plain sight; examples include the verbose densely-written clinical letter that never comes to the point, the imaging report that lists only one diagnostic possibility when several are possible (or which irritatingly avoids any interpretation at all) and the critical pathology result buried among others, or presented in a way that does not highlight its importance.
These represent failures to put information into context. They prevent the person receiving the information from forming a judgement on its significance and can be as harmful as omitting to give information altogether. Certainly they make the information recipient’s job more difficult.
The term “failure of communication” has unfortunately been degraded through its use as a euphemism for “interpersonal disagreement” (or “bust up” if you prefer). In many such cases people are communicating only too well!
How much information is “enough”?
Earlier I referred to the dangers of the verbose, densely-written clinical letter. Presenting others with the facts, giving your opinion about what you think those facts add up to, and suggesting how you might use the information, is a key part of sound clinical communication.
The opposite is to dump the unfiltered data into the recipient’s lap and leave them to get on with sorting out the problem. I need say no more about what kind of reaction that is likely to produce!
The US Navy came up with the SBAR system (see below) to create consistently-sound communication at sea.
The system was adapted to communications between healthcare professionals by Dr Michael Leonard and co-workers Doug Bonacum and Suzanne Graham at the Kaiser Permanente organisation in Colorado, USA.
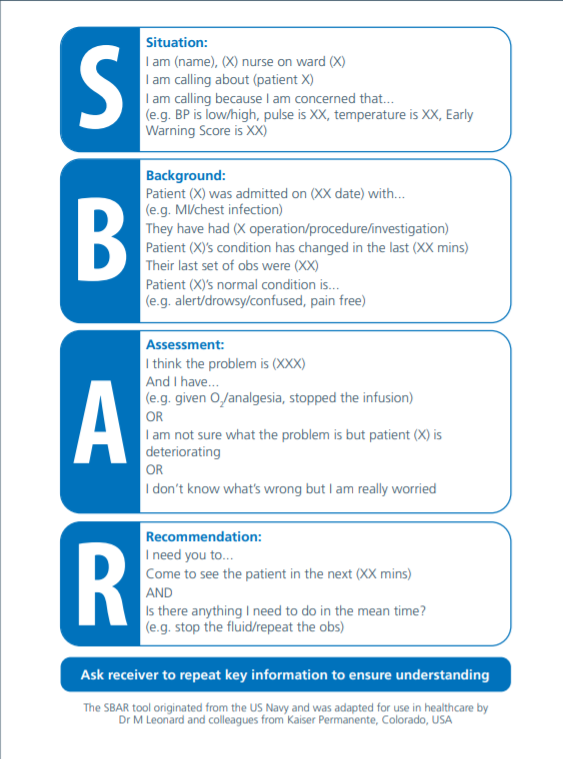
The above version of the SBAR diagram is taken from an NHS England and NHS Improvement document .
SBAR lends itself particularly well to verbal communication, but in my view every written clinical communication (ie letter or email) that you send to other doctors should contain the same elements as the SBAR system, with a few other features:
A brief summary of the relevant facts of the case you are describing. I prefer to use bullet points to aid readability.
A focus on information that contributes to patient management - and exclusion of information that does not contribute.
Provision of information in a way that promotes reflection by the recipient (as a way of saying “this is not all cut and dried, we need to think about this”)
A brief statement of what you think the problem is and what you plan to do about it. Mention one or two alternative possible diagnoses or management paths.
Use of the words “probably” and “possibly” when (as is often the case) there is diagnostic and management uncertainty.
Saying that you would value your reader’s opinion about your proposed action. This calls for their active support in solving the problem at hand.
I recall an example of the opposite of this approach that I found particularly irritating and disrespectful to both the patient and to colleagues. A radiologist reported an isotope bonescan skeletal survey in just two words: “multiple metastases”.
Sadly the report proved to be correct. However I could not assume that, because a few months earlier I had seen another patient with similar appearances on their isotope bonescan who turned out to have a more benign condition (hypophosphataemic osteomalacia due to renal tubular disease).
Multiple hotspots on the isotope bonescan may also be seen following repeated and widespread severe skeletal trauma.
My advice is that you should not accept terse, rigidly-worded reports like that. You should instead have them reviewed in their clinical context at a meeting involving suitably-experienced radiologists.
Electronic Patient Records (EPRs) both facilitate and impede information transfer
The use of EPRs has considerably helped patient administration, with fewer lost followups and bookings.
EPRs also assist with information transfer between health professionals because EPR entries are much easier to index by date and speciality than entries in large files of paper notes. This speeds up the search for relevant entries.
However the design of the EPR systems that I have encountered leaves a lot to be desired; entries are displayed in time order under speciality headings, but often with no clue to their contents. Sometimes one has to sort through other parts of the EPR to find pointers to relevant entries.
In busy clinical practice this is a disincentive to search the EPR.
I think it likely that EPR clinical notes will eventually be displayed in speciality clusters in a touchscreen (or clickable) format, each cluster with its own onscreen drop-down menu listing the category of contents of the speciality cluster such as ward round notes and outpatient attendances.
Wording of x-ray requests and referrals to other specialties:
Your referrals to other specialities will be better received if you make them short, to the point and clear about what you would like the other speciality to consider. You are transferring information in digestible form to these specialities, not writing an elegant letter!
I recommend the use of bullet points if the data format of the requesting system allows thesec
Referrals to imaging and histocytopathology departments illustrate this point. Doctors in both of those specialties need adequate clinical information in order to produce an adequate differential diagnosis of the appearances seen.
You should thus give the patient’s age and gender, with a very brief time-framed summary of the relevant history to orientate the reader (eg “60 year old plumber, smoker, previous myocardial infarct, with recent onset dyspnoea” rather than “this gentleman presented with shortage of breath on walking uphill”).
This should be followed by questions that need to be answered: ?cardiomegaly ?interstitial oedema ? consolidation? pleural effusion/ thickening
You must include relevant geographical context eg “ 45 year old man from a developing country, 3 month history of cough, loss of weight, smokes 40 cigarettes a day” on a chest x-ray request orientates the radiologist to possible diagnoses of tuberculosis and lung cancer.
The alternative is simply to list the diagnoses that you would like the specialist to consider.
Meeting with GPs
The increased clinical workload in the UK since the start of the recovery from the Covid-19 pandemic has highlighted longstanding problems in communication between hospital doctors and GPs.
Years ago GPs and hospital doctors met frequently at professional and social gatherings that often included semi-formal professional updates.
Over recent years these gatherings have become less frequent due to work pressures, shift working and part-time working, and because of the expansion of other forms of continuing professional development.
Meetings between doctors working in primary and secondary care have become even less frequent during the Pandemic, other than those at a managerial level which involve few doctors.
These developments mean that it is now more difficult than ever for individual doctors on both sides of the hospital-community divide to know what their colleagues on the other side are thinking.
Letters to GPs
When writing to GPs you should remember that your letters are not always being acted on by medically qualified personnel. You thus need to give crystal -clear, unambivalent information.
A helpful letter format for physicians has become widely used in the UK in recent years. This involves starting your letter with a numbered list of active diagnoses - conditions which are currently active, or which may impinge on the patient’s treatment, or on their other active conditions. A hernia repair 40 years ago is not an active diagnosis unless the patient is presenting with abdominal symptoms.
You should then give a list of medications that you have confirmed with the patient. Please bear in mind that many patients cannot remember exactly what they are taking. Doses of drugs should be given when relevant (especially for drugs like prednisolone).
Short sections covering the relevant history and examination then follow.
I find it useful to sum up with an Assessment section in which I give my impressions of what is causing the patient’s symptoms, whether the patient’s condition is improving or worsening and the evidence and reasons for my conclusions.
I always conclude with a Plan in which I make clear to the GPs what I am asking them to do about the patient’s condition. Similarly I state clearly what I am planning to do.
Agree to distribute the workload
It has become more clear (if it were ever in doubt) that poor communications between primary and secondary care are contributing to safety risks and inefficiencies that include delays and duplication of clinical and administrative activity.
The decline in the number of general practitioners in the UK over recent years and the steadily-growing number of patient attendances has made it more difficult for patients to have consultations with what they regard as their own GPs.
As a result those patients who also attend hospital clinics frequently wish to discuss problems that in the past they would have discussed with their GPs, on the offchance that the hospital doctor (often a physician) may be able to provide a solution. This in turn stresses hospital staff attempting to provide services for which they are not equipped.
Recent GP contracts are compelling hospital doctors to follow up their own activity and advice. This includes initiating prescriptions and investigating abnormalities that they have identified, which could be linked to the condition for which they see the patient.
These constraints require the exercise of fine judgement by you as a hospital doctor in deciding which tasks to do yourself and which to pass across to the GP. The individual patient’s welfare should always be the deciding criterion.
You must avoid the situation where (for example) you have asked a patient’s GP to follow up on anaemia identified on routine speciality blood tests, then discover many months later, when the patient presents with late stage colon cancer, that the GP did not receive your message. You could easily have avoided that situation at little cost in time and effort by starting the investigations yourself.
Possible solutions to hospital-community communication problems:
Solutions to the communication difficulties between primary and secondary care are no doubt already in place in some areas. I very much hope that development of such collaborative solutions will become a core feature of the new NHS Integrated Care Systems (ICSs), which are designed to improve hospital-community links.
These collaborative solutions should primarily aim to deal with clinical communications issues although the best-designed informatics systems should also be able to deal with many managerial data concerns such as numbers of patients seen, waiting times etc.
The solutions must allow rapid and straightforward analysis and audit of often-large amounts of clinical data, with solid privacy protections.
The development of these solutions should take place in small achievable steps within an overall strategy aiming for integration of all types of hospital and community clinical data, and of relevant social care records.
These steps should be based on the advice of the systems’ users namely the GPs, other community specialists, hospital specialists, social care providers and other healthcare providers. In some situations a structured approach to collecting and analysing their opinions may be useful, including a Delphi analysis.
Excellent leadership of the whole process is obligatory.
Examples of solutions include:
Common EPRs for hospital and community services into which information can be entered and read simultaneously by all permitted parties.
Limited-character secure messaging between specialists and GPs from phone or desktop apps, with messages about patients filed automatically in their EPRs to create an audit trail and to allow highlighting of particularly important messages.
Smartphone apps for direct patient-specialist department communication with analysis of outcomes and of time devoted to responses by specialist teams.
Easily- usable systems for transferring the pathology results of out of area patients and of patients moved from other hospitals. Effective if somewhat-cumbersome methods already exist for transferring PACS images between some hospitals.
Widespread use of graphing of pathology results to identify emerging trends in data such as falling neutrophil counts and rising creatinine levels, with trend reports sent automatically to both hospital and community practitioners.
Short MDT – style videoconferences held between GPs and small groups of hospital specialists to find solutions in cases where communication problems have impaired management.
Doubtless there are many other examples which could be suggested by individual users.
In conclusion, the NHS is not capitalising as effectively as it might on the vast amount of information that it generates. Communications are fragmented where they should be more centralised, and sometimes centralised where they should be localised and regionalised.
Improvements in safety, efficiency and personalisation of patient care will almost-certainly follow an improvement in clinical communication systems.
Meanwhile we doctors can make our own lives easier by observing a few simple principles that I have detailed in this post.
Next blog: Leadership and teamwork in internal medicine.